March month is commemorated for spreading awareness of colorectal cancer (CRC) which according to recent reports from the World Cancer Research Fund (WCRF), is today the third most common malignancy and the fourth leading cause of cancer-related deaths in the world. CRC is the third most common cancer in men and the second most prevalent cancer in women and the incidence is high in countries like Hungary, Norway and Korea. Data also indicates that for the year 2018, over 1.8 million new cases of CRC were diagnosed. The worrying observations are that by the year 2030, the global burden of CRC is expected to increase by 60% to more than 2.2 million new cases and of these nearly 1.1 million people will succumb to the illness deaths and that nearly 60% of this will be in the developing countries that have minimal resources to manage.
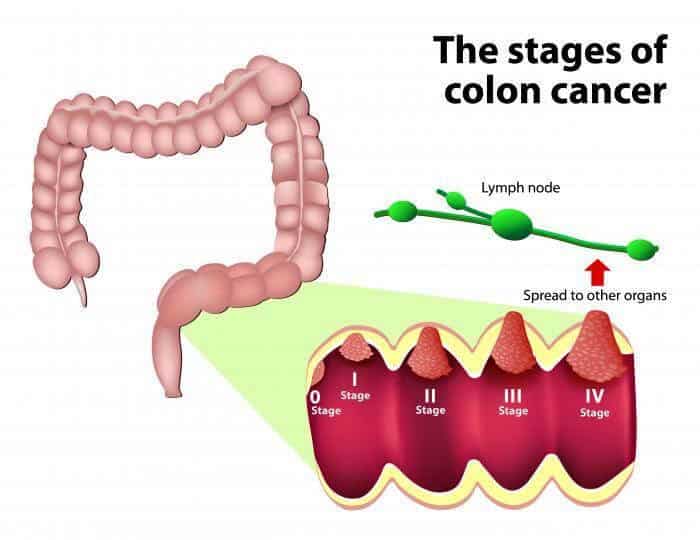
From a medical angle, cancer arising from the large intestine is referred to as colorectal cancer. They usually start in the innermost layer (mucosa) and can grow through some or all of the tissue layers that make up the colon and rectum. The extent to which cancer penetrates the various tissue layers determines the stage of the disease. Most colorectal cancers begin as a polyp, a growth in the tissue that lines the inner surface of the colon or rectum. The polyps may be flat, or they may be raised. Raised polyps may grow on the inner surface of the colon or rectum like mushrooms without a stalk, or they may grow like a mushroom with a stalk. Polyps are common in people older than 50 years of age, and most are not cancer. However, a certain type of polyp known as an adenoma may have a higher risk of becoming a cancer.
Causes for CRC:
As with other cancers, the exact cause/s for the initiation and development of CRC is conclusively not proved. However studies have shown that the major risk factors for CRC are family history of the disease and older age, and several other factors like excessive alcohol use, obesity, being physically inactive, cigarette smoking, and diet have been associated with increased risk. The details are enlisted here with.
- Inherited gene mutations: Multiple studies have now shown that inherited gene mutations that increase the risk of colon cancer can be passed through families. However what is important to remember is that inherited gene mutations don’t make cancer inevitable, but they can increase an individual’s risk of cancer significantly. The most common forms of inherited colon cancer syndromes are hereditary nonpolyposis colorectal cancer (HNPCC) also called Lynch syndrome, which increases the risk of CRC in people below the age of 50. The other important inherited gene mutation is the familial adenomatous polyposis (FAP), rare disorder that causes development of thousands of polyps in the lining of the colon and rectum and thereby increases risk of developing colon cancer before age 40.
- Older age: Globally majority of people diagnosed with CRC are older than 50. CRC can occur in younger people, but its incidence is much less.
- Human race: African-Americans have a greater risk of colon cancer than do people of other races.
- Personal history of colorectal cancer or polyps: If a person already has colon cancer or adenomatous polyps, then there is a greater risk of developing CRC in the future.
- Inflammatory intestinal conditions: Chronic inflammatory diseases of the colon, like ulcerative colitis and Crohn’s disease significantly increase the risk of development of CRC.
- Sedentary lifestyle: People who are inactive and sedentary are more likely to develop CRC. Adopting regular physical activity may reduce the risk of colon cancer.
- Diabetes: People with diabetes and insulin resistance are at increased risk of developing CRC.
- Obesity: when compared with people considered normal weight, people who are obese have an increased risk of colon cancer and an increased risk of dying of colon cancer.
- Smoking: when compared to non smokers, people who smoke may have an increased risk of colon cancer.
- Alcohol: when compared to people who do not drink alcohol, heavy use of alcohol increases the risk of CRC.
- Diet: The diet of an individual plays an important role in the development of CRC. Studies have now shown that a diet rich in processed red meat and low in fiber increases the risk of colon cancer.
Signs and symptoms:
Like most cancers, CRC might not cause symptoms right away and many of the symptoms can also be caused by ailments that are not cancer like infection, hemorrhoids, irritable bowel syndrome, or inflammatory bowel disease. The most common signs include:
- Change in bowel habits, such as diarrhea, increasing constipation or increasing requirement of laxatives and narrow calibre of stool that lasts for few days/weeks/ months.
- Constant or frequent urge to have bowel movements, which still persist even after passing stool
- Rectal bleeding, dark stools, or blood in the stool
- Stools that is thinner than normal and with foul smell
- Abdominal bloating, cramps or discomfort and pain
- Weakness and fatigue
- Decrease in appetite and unexplained significant weight loss within few weeks.
However when the cancer has metastasized and spread outside the colon or rectum region, the signs are organ specific and include:
- Pain, fractures, constipation and/or high calcium levels when bones are involved.
- Shortness of breath, difficulty breathing, coughing, pain and/or fatigue when the lungs are affected.
- Nausea, fatigue, swelling of the feet and hands, increased abdominal girth and/or jaundice when the liver is affected
- Bloating, swollen belly and/or loss of appetite when the lymph nodes of the abdomen are affected.
- Pain, confusion, memory loss, headache, blurred or double vision, difficulty speaking and/or seizures when the brain and/or spinal cord are affected.
Cancer screening:
Screening means examining people without symptoms in order to detect disease or find people at increased risk of disease. It is often the first step in making a definitive diagnosis. For colorectal cancer screening, its purpose is to find people who have colorectal cancer, before they have any symptom, in order to offer them earlier treatment. The early diagnoses through screening are very beneficial as it is easier to treat. Further, removing the pre-cancerous growths (polyps) is highly beneficial as it prevents the forming of colorectal cancers. The American Cancer Society recommends that adults age 45 to 75 be screened for colorectal cancer regularly, while those above the age of 76 should ask their doctor if they should be screened. The common screening tests for colorectal cancer include fecal occult blood test (FOBT), sigmoidoscopy and colonoscopy. Newer technologies such as virtual colonoscopy and stool DNA test (sDNA) are emerging as potential options for colorectal cancer screening. The three most common methods used in India are.
- FOBT is commonly called a stool test, which can be carried out at home with instructions followed. It detects hidden blood in stool samples, even in tiny amount. The presence of hidden blood indicates bleeding somewhere in the bowel. FOBT is recommended every one to two years and when positive, colonoscopy needs to be performed.
- Sigmoidoscope is a scope with a video camera which is about 60cm in length. Doctors use it to examine the wall of large bowel by inserting it from the anus. The range of examination is up to the lower portion of the colon. Bowel preparation and low residue diet are needed. Sedative drug and pain-killer may be injected right before examination to reduce patients’ anxiety and any discomfort. During sigmoidoscopy, doctors can also obtain tissue samples for laboratory examination and remove any polyp.
- Colonoscopy is currently the best method to examine the lower digestive tract. With the scope length of 1.6 m, it helps to inspect the entire colon. Usually it takes about 15 minutes to 1 hour for the procedure. Colonoscopy every 10 years is the most preferred CRC screening strategy. Sedative drug and pain-killer are injected right before examination to reduce patients’ anxiety and any discomfort. Tissue samples for laboratory examination will be obtained and polyps can be removed during colonoscopy.
Treatment for CRC:
Like with most cancers the choice of treatment for CRC depends on the stage of the disease and the general health of the individual. The most important aspect considered is whether the cancer is localized or spread to organs like liver, lungs or some other parts of the body. The treatment options primarily include surgery, radiation therapy and chemotherapy either alone or in combination. Surgery forms the mainstay of treatment for colorectal cancer when the tumor is localized to the colon or rectum, while chemotherapy is primarily used when the cancer has spread. In addition to this, depending on the stage and the tumor location, radiation is also used to reduce the tumor size before surgery and/or after surgery to kill the remainder cancer cells.
Dr Suresh Rao the Director of Mangalore Institute of Oncology stated that colorectal cancers are common in India and that complete cure is possible when the cancer is detected early. He also said that MIO has developed a refined version of radiation treatment for rectal cancers (http://www.daijiworld.com/news/newsDisplay.aspx?newsID=413906) and that the results are very encouraging. Dr Rao opined that certain lifestyle modifications can help prevent or decrease the chances of getting this cancer and that adopting healthy food habits like eating high fiber diet, avoiding or limiting intake of fat and processed red meat, cessation of smoking and alcohol consumption and increasing physical activity through regular exercise.